July 2022
Preop image

Preop Clinical fx abutment
The patient presented for a second time for retrieval of a second fractured abutment in a Neodent CM 5.0 implant in the #19 site. The first fractured abutment recovery occurred on 10.29.20 with the implant placement date of 06.10.2019 and original restorative placement on
10.03.2019. The fracturing interval was about one year in function for the first fracture and a little over 2 years for the second. The trend isn’t encouraging and expensive for all involved.
The second recovery of the fractured abutment was accomplished in the manner as the first recovery. The crown was removed to expose the implant top. The most time efficient and safest method is to clear the throughbore to the depth of 3mm, tap the conical fragment and then distract the fragment prior to retrieving the screw fragment. Therefore, after explaining the process, the tissue was infiltrated, and conservative access was achieved to expose the implant top circumferentially. The abutment screw shaft was reduced to the top of the implant by reducing the outside diameter which forces the screw up as much as possible. Then, with a 1.25mm twist drill, the screw shaft was reduced further to the depth of 3mm. This process actually pushes the screw down, so obtaining 3mm of clearance does not require drilling all 3mm. This was done with microscope guidance, taking care to remain as concentric as possible to preserve the conical fragment wall. After completion, the existing bore was tapped to M1.8. The threads achieved were high quality and a custom made M1.8 distraction bolt engaged well. The distraction nut was engaged into the distraction bolt and the conical fragment was recovered from the implant. With the abutment interface clear, the residual abutment screw fragment was quickly retrieved, the implant was cleaned, and the supplied healing abutment was delivered finger tight.
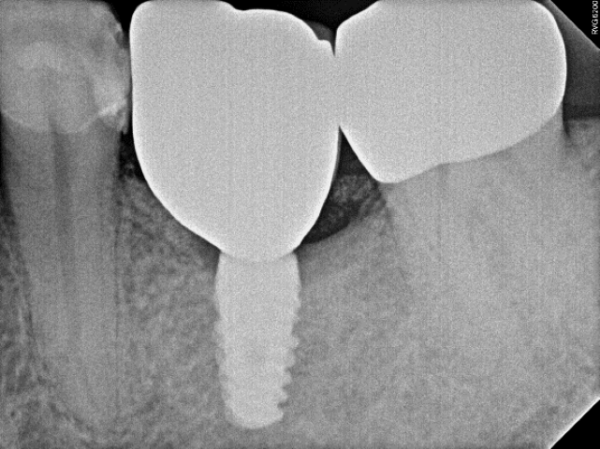
Postop – implant clear
So why has this abutment fractured twice?
This Neodent CM implant is basically a modified clone of the Ankylos C/X implant and unfortunately has the same mechanical limitations. Due to the basic design and the use of one interface ported into all implants from 3.5mm to 7mm, the fractured abutment cross-section is very thin as it emerges from the implant. When the restoration is subjected to torsional loading, fractures propagation occurs in this weakest cross-section. Predictably, this occurs in both Ankylos and Neodent CM systems. This extra loading occurs mainly in molar applications where the torsional loading is the greatest. This is due to the combined result of increased size of the occlusal tables, which increases the torsional loading forces due to longer leverage arms and increased bite force, due to the efficiency of the physics of the masticatory system. Remember, torsional loading is simply the equation of “force x leverage arm” and the compounding of the force is absolutely amazing. The outside diameter of the abutment at the implant top is 2.5mm but the cross-sectional area is reduced by the throughbore for the abutment screw. The Ankylos C/X implant abutment has a reduced diameter throughbore of 1.11mm, but the Neodent CM design has an abutment screw throughbore of 1.51mm.
This might not seem like a big difference, but this reduces the abutment titanium cross section at the point where the abutment always breaks, at the implant top, from 3.941sq.mm in the Ankylos implant to 3.118sq.mm in the Neodent CM. This is approximately a 21% decrease in cross-sectional area. In all of the abutment fractures I have treated, the only smaller cross section, as an abutment emerges from the implant, that I have measured is in a non-OEM Glidewell abutment for this interface. This abutment design, avoids the reduced diameter throughbore, having a 1.78mm throughbore and therefore has 2.421sq. mm of titanium in the cross section, a 38.5% reduction in surface area. These numbers are pitifully small, and to put this into better perspective, a Straumann RC 4.1 or 4.8 interface has a cross section of 6.11Sq.mm in the same critical area. The Dentsply Astra EV 4.2 in the same cross-section has 7.07sq.mm, while the Dentsply Astra 4.8 EV has a cross sectional area of 9.96sq.mm. This simple analysis is irrefutable, and it is absolutely no wonder why this implant abutment has suffered two fractures in 3 years. There is a solid abutment that can be placed but doing the same analysis on it yields a cross sectional area of 4.91sq.mm. While this is better, I have recovered numerous fractured solid Ankylos abutments, so using a solid may delay another fracture for a bit longer, but I don’t believe using it will take the fracture problem off the table. As this is a single tooth implant and the adjoining teeth are stable there is no possibility to look for help with splinting. The only true fix is to start over, and in fact we have done this with several Ankylos cases where patients have fractured the Ankylos solid abutment in a short time period and there is no way to dissipate the torsional load with splinting to protect this weak cross section. Sort of game, set, match. If that approach is being considered, and as pointed out above, think carefully as to what implant system and diameter the replacement will be to avoid yet another future disappointing mechanical failure. CAM





