February 2022
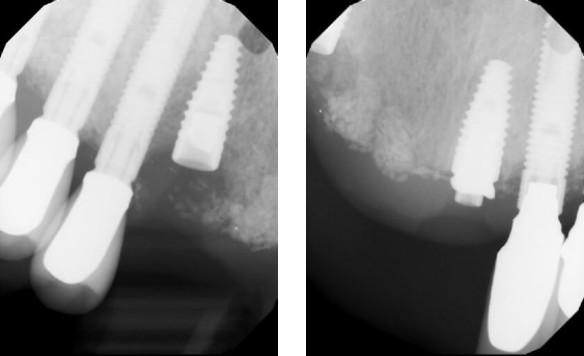
Preop images from the restorative Dr. of #6 and #9
The patient presented on referral for retrieval of a fractured zirconia abutment from a Straumann 4.1 BL implant in the #6 site. This implant was restored with a 4-tooth fixed partial denture on implants #6 and #9. The abutments were Straumann TiBase abutments with the restorative placed in May of 2018. Per the initial intake and the patient, there were two previous recovery efforts with one doctor of about one hour each and then two another. Evidently there was discussion of procuring the Straumann recovery set to help but the availability was delayed. After the initial discussion regarding recovery protocols attention was initially focused on #6 to recover the zirconia abutment fragment. This was successfully completed, without rotary instruments, by “wobbling” the majority of the fragment out with a precision fitting tool which utilized the throughbore of the fragment. There were two residual rings of zirconia visualized at 25x, but they were removed with an endodontic explorer and some patience. When the internal aspect of the implant was cleaned and examined it was easily determined that the original abutment screw had fractured just below the first implant thread and there had been some inadvertent implant thread damage, probably from one the previous zirconia retrieval attempts. This was clearly done with a rotary instrument and in retrospect there were two areas, one at 12:00 the other at 1:00, which can be visualized on the second preop 25x microscope image below. The recovery then shifted from a zirconia abutment recovery to a screw fragment recovery. The screw was found to be below the first implant thread and not mobile which makes it a Type IV recovery in my protocol algorithm which required concentric mobilization by drilling and then retrieval, hopefully avoiding a complete drill out. A precision custom drill guide was fitted and stabilized posteriorly with Triad gel after concentric dimpling the fragment with a SL ¼ round highspeed at 16x. The initial drill used was custom .8mm drill turning counterclockwise with concentricity confirmation several times. Fortunately, the fragment dislodged onto the drill and the implant was then free of debris. As there was notable thread damage, a M1.6 tap was then passed thorough the threads to ensure patency. As it is difficult to access exact thread damage though the microscope, a polyvinyl impression was taken of the internal implant which can be viewed below in 4 views which are at 90-degree rotations. From the 4 views the tread damage can be clearly accessed. There are 5 threads in a Straumann RC implant and this one has about 50% of the first thread missing and a portion, maybe 30%, of the second thread. The remaining threads are intact. There was no visible damage to the crossfit connection or the lead in .9mm, 15-degree bevel. For completeness, the healing abutment was removed and #9 was cleaned, microscopically examined, and found to be free of defects at the 25x visual inspection level. There is an image of this implant below which can be compared to the final image of #6.
I would think the mechanism of failure was a fractured zirconia abutment in #6 followed by the abutment screw fracture, possibly because the zirconia could not handle the lateral torsional loads in right lateral movements. This leads into the potential restorative plan to replace the restoration. First, I believe zirconia should be avoided, and titanium custom abutments used instead. Second, consideration to make this restoration screw retained so there is easy access to the abutment screws in the event #6 loses preload secondary to some of the threads missing and the basic nature of the Straumann cross fit joint. Consideration should also be given to double abutting the restoration as both ends have single tooth implant restorations which could add significant stability.
Lastly, when attempting a retrieval as in this case, I would highly recommend to not introduce rotary instruments without microscope guidance. The dimensions are small, and the tolerances are tight, and things can and will head south quickly. Even though very precision guidance was used to recover the abutment screw fragment the microscope was used to make sure each step was on target. Have a look at the precision drilling through the screw fragment which will confirm the above. I often say you think you can see it with loops, but you can truly understand the situation at hand with the scope. This case was clearly made more difficult by the previous uncontrolled retrieval efforts by not having the proper visualization or recovery protocols and experience.



3 Preop clinical views of the zirconia fragment and in the right 2 images the reflection at 12:00 and 1:00 are implant defects from zirconia drilling











Impression of the implant threads at 90-degree rotation: note the 5 original threads on the left image and the thread loss in the top two threads as the impression rotates



Recovered screw fragment on the .8mm custom drill: note the concentricity away from the threads as the drill tip exited the screw end





